INN & Regulatory Reference
NexCAR19™
A New Hope for Hard to Treat B-Cell Cancers
An Overview of NexCAR19™
A breakthrough in precision oncology, NexCAR19™ (Talicabtagene autoleucel) is a second-generation, autologous, CD19-directed chimeric antigen receptor (CAR) T-cell immunotherapy. Built on a fully humanized molecular platform, it is precision-engineered to address the critical unmet need in relapsed or refractory B-cell malignancies.
NexCAR19™ is a prescription therapy indicated for specific relapsed or refractory B-cell Non-Hodgkin’s Lymphomas and B-cell Acute Lymphoblastic Leukaemia in patients whose frontline or other standard treatments have been unsuccessful.
CDSCO Approved
NexCAR19™
Talicabtagene autoleucel
India's first humanized
CAR-T cell therapy
CAR-T cell therapy
Developed at IIT Bombay
INN
Talicabtagene autoleucel
Type
Autologous CAR-T cell therapy
Target
CD19-directed
Generation
Second-generation
Indication
Relapsed / Refractory B-cell cancers
Eligibility
Age 15+ · ≥1 prior line of therapy
Route
Single intravenous infusion
Approval
CDSCO approved - India
47%
B-NHL
1 Year PFS
55%
B-ALL
1 Year PFS
3+
Years
Longest Remission
Longest Remission
Duration of Response
98%
Manufacturing
Success Rate
Success Rate
Commercial batches
~18 Days
Manufacturing
Turnaround
Turnaround
Fastest in class (India)
NexCAR19™ (Talicabtagene autoleucel) - Approved Indications
B-NHL
Relapsed/Refractory B-cell Non-Hodgkin Lymphoma (R/R B-NHL)
After 1 or more lines of prior systemic therapy · Age 15 years and above
- ✓ Diffuse Large B-cell Lymphoma (DLBCL)
- ✓ Primary Mediastinal B-cell Lymphoma (PMBCL)
- ✓ Follicular Lymphoma (FL)
- ✓ Mantle Cell Lymphoma (MCL)
- ✓ Marginal Zone Lymphoma (MZL)
- ✓ High-Grade B-cell Lymphoma (HGBL)
Epidemiology Context
~40% of DLBCL patients relapse after first-line therapy; >60% are ineligible for autologous stem cell transplantation (ASCT), representing a significant unmet need addressed by NexCAR19™.
B-ALL
Relapsed/Refractory B-cell Acute Lymphoblastic Leukemia (R/R B-ALL)
After 1 or more lines of prior therapy · Age 15 years and above
- ✓ CD19-positive B-cell precursor ALL confirmed by flow cytometry or immunohistochemistry
- ✓ Relapsed or refractory after ≥1 prior line of therapy, including one intensive chemotherapy regimen
- ✓ Applicable to adolescents (age 15–18) and adults - broadening access vs. paediatric-only CAR-T therapies
- ✓ No active CNS involvement at time of treatment (CNS-1 or CNS-2 only after clearance)
Epidemiology Context
Historical B-ALL survival after relapse remains poor at ~41% with conventional chemotherapy. NexCAR19™ provides a curative-intent option where allogeneic SCT may not be feasible or accessible.
NexCAR19™ was assessed in an open-label, multicentre, phase 1/2 study in six tertiary cancer centres across India. Of 64 patients aged 15 and above with either relapsed/refractor B-cell lymphoma or B-cell acute lymphoblastic leukaemia, 14 were enrolled in Phase 1, and 50 were enrolled in Phase 2. At an efficacy dose of at least 5 × 10⁶ CAR T cells per kg of body weight, NexCAR19 demonstrated an overall response rate of 73%. The trial exhibited a manageable safety profile with high efficacy in a difficult-to-treat population with B-cell malignancies, with these results published in Lancet Haematology
Unmet Needs in Relapsed/Refractory B-Cell Malignancies
Transforming outcomes for patients with relapsed/refractory B-cell malignancies – where current treatments fall short. Despite significant advances in oncology, a large proportion of patients relapse after frontline therapy, and for many, curative options remain out of reach. These numbers reflect the scale of the challenge and the urgent need for more effective, accessible treatments.
01
>550,000
Global B-Cell Malignancy Burden
More than 550,000 new B-cell non-Hodgkin lymphoma cases and over 100,000 B-ALL cases are diagnosed globally each year - representing one of the largest unmet burdens in oncology.
Source: GLOBOCAN 2022; PMC11829893
02
30 - 40%
Relapsed / Refractory Disease
Up to 40% of DLBCL patients and 20-25% of ALL patients develop relapsed or refractory disease after frontline therapy - with minimal durable responses to standard salvage regimens.
Source: ASCO EDBK_390802; Tandfonline 2024
03
>60%
Limited Access to Curative Therapies
More than 60% of patients with relapsed DLBCL are not eligible for stem cell transplant due to age, comorbidities, or chemo-refractory disease. Median survival with conventional therapy is only ~6 months.
Source: Semanticscholar; PubMed 30213390
04
~90,000
India's Growing Disease Burden
India reports ~50,000 new leukemia and ~40,000 NHL cases annually. Only 0.09% of India's population is registered as potential stem cell donors - a fraction of rates in Western countries.
Source: GLOBOCAN 2022 India; PMC11893321Patient Journey - HCP Workflow
A coordinated 5-step process from eligibility confirmation to infusion and monitoring
1
Eligibility Assessment
Evaluate diagnosis, disease status, prior lines of therapy, and performance status. Confirm lab criteria and contraindications. Complete pre-screening checklist.
2
Slot Scheduling
Contact ImmunoACT Local Patient Navigator/Medical Partner to schedule leukapheresis slot. Confirm patient stability, plan washout periods, and bridging therapy if required.
3
LSM Collection
Leukapheresis at a certified apheresis centre (~4–6 hours). PBMCs collected and transported via ImmunoACT's coordinated logistics. Fresh refrigerated pickup.
4
Manufacturing
~18-day GMP manufacturing at ImmunoACT facility. 98% success rate. Notifications provided at LSM acceptance, in-process QC, final QC, and dispatch.
5
Infusion & Monitoring
Confirm fitness for lymphodepletion. Single IV infusion (~30 minutes). Structured post-infusion monitoring with CRS/ICANS management per protocol.
 Important: This workflow represents a generalized treatment pathway. Patient-specific variations in sequencing, timelines, and interventions are expected and are determined by the treating oncologist/haematologist based on disease progression, clinical status, and institutional protocols.
Important: This workflow represents a generalized treatment pathway. Patient-specific variations in sequencing, timelines, and interventions are expected and are determined by the treating oncologist/haematologist based on disease progression, clinical status, and institutional protocols.Recommended Patient Eligibility Criteria
Assess all criteria before initiating the NexCAR19 treatment process.
General Eligibility Criteria
- ECOG Performance Status: 0–2
- Ejection Fraction ≥45% (2D Echo, within 6 weeks)
- Peripheral Blood ALC ≥500/μL or Absolute CD3+ T cell count ≥150/μL
- AST/ALT ≤3× ULN | Total Bilirubin ≤2× ULN
- Creatinine Clearance ≥30 mL/min
- Well-preserved lung function
- Well-controlled pre-existing comorbidities
- Negative viral markers (HIV, HBV, HCV, CMV)
- CNS disease well-mitigated if involved
- Absence of active infection or acute inflammation
Evaluate carefully:
- Active uncontrolled infections or acute inflammation
- Uncontrolled or severe cardiac conditions
- Pregnancy or breastfeeding (contraindicated)
Disease-Specific Criteria
- After 1 or more prior lines of therapy
- Age 15 years and above
- Relapsed or refractory after standard lines of therapy
- CD19-positive confirmed by flow cytometry or IHC
- Measurable disease per Lugano criteria at screening
- Prior ASCT patients may be eligible — evaluate case-by-case
- Leukapheresis feasibility and timing confirmed
- No active CNS lymphoma at time of treatment
~40% of DLBCL patients relapse after first-line therapy. NexCAR19 demonstrated 72% ORR at 28 days in this population.
Patient Journey Overview
Step 1: Eligibility Assessment
Determine Suitability for NexCAR19 Therapy
Evaluate the patient against NexCAR19’s eligibility criteria, including diagnosis, disease status, prior lines of therapy, and performance status.
Step 2: Slot Scheduling
Coordinate Leukapheresis Timing Based on Clinical Readiness
Once eligibility is confirmed, our team will contact you to schedule a leukapheresis slot at your facility or designated center.
Please ensure:
-
Patient is clinically stable and fit for leukapheresis
-
Appropriate drug washout periods are observed
-
Any bridging therapy is planned with manufacturing timelines in mind
Step 3: LSM Collection
Timely & Controlled Pickup of Leukapheresis Material
Upon successful leukapheresis:
-
ImmunoACT or its certified logistics partner will coordinate fresh refrigerated pickup of the Leukapheresis Starting Material (LSM)
-
Ensuring correct labeling, documentation, and chain-of-custody protocols are followed
Step 4: Manufacturing
Stay Informed at Key Checkpoints During Manufacturing
You will receive notifications at the following stages:
-
LSM acceptance and initiation of manufacturing
-
Completion of in-process and final quality checks
-
Expected product readiness and dispatch timeline
Step 5: Infusion & Monitoring
Product Delivery, Infusion Scheduling, and Post-Infusion Care
NexCAR19 will be delivered in advance of your selected infusion window:
-
Confirm patient’s fitness for lymphodepletion and infusion
-
Administer NexCAR19 as per prescribing information
-
Follow structured monitoring protocol post-infusion, including CRS/ICANS management if needed
What are the Side Effects of NexCAR19?
NexCAR19™ may cause side effects that are severe and/or life-threatening.

Fever (100.4°F/38°C or higher)

Difficulty breathing

Chills or shaking chills

Confusion

Dizziness or lightheadedness

Severe nausea, vomiting, or diarrhea

Fast or irregular heartbeat
Severe fatigue or weakness
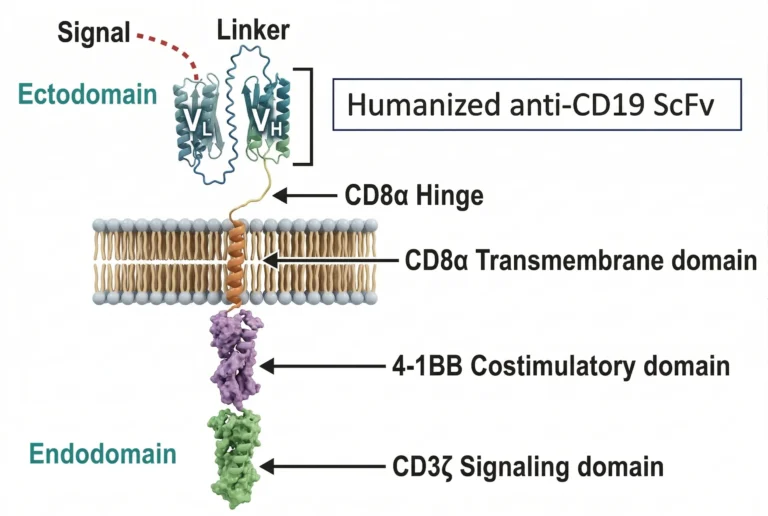
How does NexCAR19™ work - Scientific Profile
A humanized CD19-targeting CAR-T construct with optimized persistence and reduced immunogenicity
-
Humanized scFv — CD19 TargetingA humanized single-chain variable fragment (scFv) antibody specifically targets CD19 markers on B-cells. Humanized design significantly reduces immunogenicity compared to murine-based CAR constructs.
-
Optimized Flexible Spacer (CD8 Hinge)An optimized flexible spacer enhances target binding efficiency and allows optimal orientation of the scFv for CD19 engagement.
-
4-1BB Co-stimulatory DomainSpecialized 4-1BB co-stimulatory signaling significantly boosts T-cell activation and promotes long-term T-cell persistence — contributing to durability of response beyond 24 months in select patients.
-
CD3ζ Signaling DomainCD3ζ signaling components trigger potent T-cell immune response upon CD19 binding, initiating cytotoxic killing of CD19+ malignant B-cells.
Proven Clinical Performance
Our anti-CD19 binding technology has demonstrated remarkable persistence in clinical settings, with documented durability of action extending beyond 24 months in select patients. The humanized ScFv component delivers exceptional efficacy while contributing to a reduced incidence of severe treatment-related toxicities.
Superior Therapeutic Profile
NexCAR19™ modified T-cells offer a comprehensive treatment solution:
- Safety: Rigorously tested cellular product with established safety profile
- Durability: Long-lasting anti-cancer activity for sustained disease control
- Effectiveness: Consistent response rates across diverse patient populations
Optimized Dosing Strategy
With an efficacy threshold of more than 5 million CAR-T cells per kilogram of body weight, NexCAR19™ achieves exceptional tumor penetration and maintains effectiveness even in challenging high-risk patient populations.
NexCAR19™ is a type of CAR-T cell therapy. T-cells are naturally made by your body as an advanced defense against viruses and cancer cells. As they mature, they develop specific connectors (receptors) to target key signals in cancer cells. However, cancers can escape the inbuilt defense mechanism of T-cells, which can lead to an increase in tumor burden and can result in the survival of cancer cells and a further increase in tumor burden. CD19 is a protein commonly present on the surfaces of certain B-cell cancers.
Our scientists have designed instructions for your T-cells to express unique proteins called Chimeric Antigen Receptors (CARs) on their surface, which will enable them to bind to a specific target on the cancer cells. These instructions are delivered genetically using a vehicle known as a lentiviral vector.NexCAR19 targets a marker called CD19, which is commonly present on the surface of cancerous B-cells.
1. Isolate
Select and activate T-cells from the patient’s blood sample.
2. Program
Deliver genetic instructions to T-cells using viral vectors.
3. Engineer
Enable T-cells to express Chimeric Antigen Receptors (CARs).
4. Expand
Multiply CAR-T cells to achieve the therapeutic dose.
5. Infuse
Administer CAR-T cells to the patient for targeted cancer treatment.
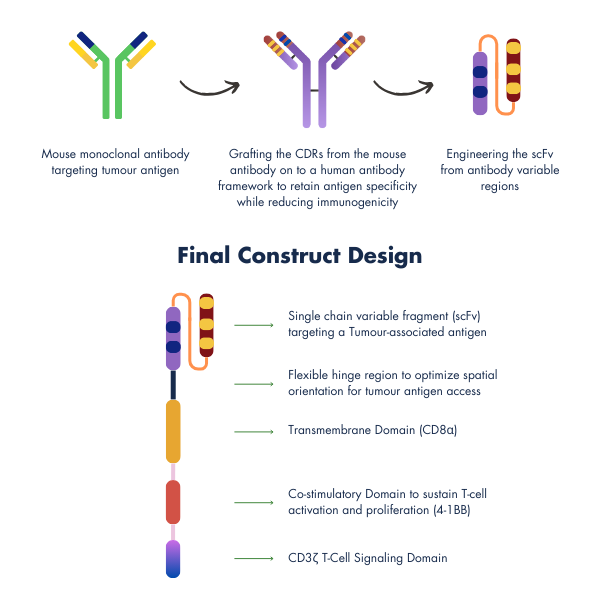
Smarter CAR-Construct & Design for Safer Treatment
At the heart of ImmunoACT’s innovation is a next-generation cell and gene therapy platform, purpose-built to deliver affordable efficacy without compromising safety. Our approach blends cutting-edge science with thoughtful design to make these therapies more accessible and tolerable.
Our CAR-T constructs use fully humanized components, making them more “familiar” to the immune system. This reduces the risk of rejection, minimizes off-target toxicity, and improves patient experience by lowering the need for intensive supportive care.
Each CAR we design includes:
- A single-chain variable fragment (scFv) tailored for precise tumor targeting
- A flexible hinge (spacer) to enable optimal antigen engagement
- A CD8α transmembrane domain for enhanced stability
- A 4-1BB co-stimulatory domain to support T-cell survival and sustained action
- A CD3ζ signaling domain to trigger strong and specific immune responses

Our CAR-T therapies integrate humanized sequences and undergo rigorous optimization to ensure potency, persistence, and safety. By reducing the likelihood of severe toxicities, we are not just improving patient safety, we are redefining how cell therapies can be delivered.
The gene sequence of the CAR construct is first integrated into a plasmid, which is then used to produce a lentiviral vector. This vector delivers the CAR gene into T cells, enabling them to recognize and attack cancer cells.
NexCAR19™ Manufacturing Process
1. Leukapheresis
Peripheral Blood Mononuclear Cells (PBMCs) are collected from the patient using leukapheresis.
This forms the foundational starting material for autologous CAR-T cell manufacturing.
This forms the foundational starting material for autologous CAR-T cell manufacturing.
2. Monocyte Depletion
Monocytes are removed from the PBMC population to reduce non-T-cell components.
This enhances T-cell purity and improves the efficiency of downstream processes.
3. T-Cell Activation
T-lymphocytes are activated using CD3/CD28 costimulatory signals in a controlled environment. This primes the cells for efficient gene transfer during the transduction step.
4: Lentiviral Transduction
Activated T-cells are genetically modified with a lentiviral vector encoding the anti-CD19 CAR. This step equips T-cells to recognize and attack CD19-expressing tumor cells.
5: CAR-T Cell Production
Following transduction, T-cells begin expressing the chimeric antigen receptor on their surface. These cells are now classified as NexCAR19—genetically reprogrammed to target B-cell malignancies.
6: Expansion to Target Dose
The CAR-T cells are cultured under GMP conditions to reach the therapeutic dose. Cell growth is monitored to maintain viability, potency, and phenotype consistency.
7: Formulation & Cryopreservation
The final CAR-T product is formulated with infusion-ready buffer and cryopreserved. Post quality checks, it is stored under ultra-low temperatures until patient infusion.
Why NexCAR19™ ?
NexCAR19™ (talicabtagene autoleucel) is a humanized CD19-directed CAR-T cell therapy approved in India for relapsed/refractory (r/r) B-cell acute lymphoblastic leukemia (B-ALL) and B-cell non-Hodgkin lymphoma (B-NHL) in patients aged 15 years and above. It is the first CD19-targeted CAR-T therapy approved for commercial use in India. Till date NexCAR19 has treated 800+ patients through clinical and commercial use.
47%
B-NHL
1 Year PFS
55%
B-ALL
1 Year PFS
63%
B-NHL
1 Year OS
64%
B-ALL
1 Year OS
27
Months
Longest remission
>98%
Manufacturing
Success Rate
~10
Hospitalization Days
Post infusion
The results above are from a multicenter, retrospective study (CTRI/2025/08/093795) that evaluated 250 patients (105 r/r B-ALL and 145 r/r B-NHL) underwent leukapheresis with intent to receive NexCAR19 between 15 November 2023 and 31 January 2025 and followed up till 31st March 2026. The result of this study is published in Blood Cancer Journal.
Safety Profile of NexCAR19™
NexCAR19™ demonstrates a predictable and manageable safety profile, characterised by low rates of severe immune-mediated toxicities and consistent outcomes across real-world settings.
Relapsed / Refractory B-ALL
n = 98
Key Adverse Events
Cytokine Release Syndrome (CRS)
7%
Grade ≥3
ICANS (Neurotoxicity)
4%
Grade ≥3
IEC-HS (Haemophagocytic Syndrome)
23%
Any Grade
Cytopenia (within 1 month)
76%
Grade ≥3
Median Hospitalization
8 days
Median
ICU Admission
9%
Of Cohort
Tocilizumab Use
69%
Median 1 Dose
Clinical Safety Observations
Low Severe CRS Burden
Only 7% Grade ≥3 CRS, indicating a manageable inflammatory toxicity profile
Low Neurotoxicity Rates
ICANS Grade ≥3 at 4% - suggests favorable neurotoxicity profile vs historical CAR-T benchmarks
Manageable with Standard Interventions
Tocilizumab required in 69% of patients, typically a single dose - most cases controlled with standard-of-care protocols
No New Safety Signals
Safety profile consistent with known CAR-T toxicities. No unexpected adverse events reported
Real-World Feasibility
Demonstrated safety across 98 patients at 37 centres in India, indicating scalability and operational feasibility
Relapsed / Refractory B-NHL
n = 128
Key Adverse Events
Cytokine Release Syndrome (CRS)
6%
Grade ≥3
ICANS (Neurotoxicity)
3%
Grade ≥3
IEC-HS (Haemophagocytic Syndrome)
18%
Any Grade
Cytopenia (within 1 month)
77%
Grade ≥3
Median Hospitalization
12 days
Median
ICU Admission
5%
Of Cohort
Tocilizumab Use
50%
Median 1 Dose
Clinical Safety Observations
Low Severe Toxicity Burden
Grade ≥3 CRS: 6% · Grade ≥3 ICANS: 3% - indicates favorable safety profile vs historical CAR-T benchmarks
Predictable and Early-Onset CRS
Median onset at Day 3 - enables proactive monitoring and timely intervention
Limited ICU Dependency
ICU admission in only 5% of the cohort - suggests manageable toxicity in real-world settings
Manageable with Standard Interventions
Tocilizumab required in 50% of patients, typically a single dose - most cases controlled with standard-of-care protocols
Feasible Across Diverse Indian Centres
Data from 128 patients across 60+ centres - demonstrates scalable and reproducible safety outcomes
Published: Findings published in Blood Cancer Journal on 16 July 2026.
Individual patient outcomes may vary.
Individual patient outcomes may vary.
The Hope Initiative - Clinical & Institutional Support
The Hope Initiative is designed to support not just patients – but the physicians and institutions who deliver care. It is an integrated operational and clinical framework built to enable safe, scalable, and outcome-driven CAR-T therapy across India.
From institutional onboarding and protocol alignment to real-time toxicity management support and long-term outcome capture – The Hope Initiative is built around your clinical needs.
01
Institutional Onboarding
Structured onboarding frameworks to establish site readiness, align clinical protocols with global standards, implement toxicity management frameworks, and build institutional capability for safe and efficient CAR-T delivery.
CAR-T Centre Enablement02
Toxicity Management Support
Access to an experienced HCP helpline providing real-time clinical guidance to managing teams on post-infusion toxicity management - including CRS and ICANS - strengthening preparedness at every stage of post-CAR-T care.
On-demand Clinical Guidance03
Vein-to-Vein Coordination
End-to-end coordination across apheresis logistics, manufacturing timelines, and infusion scheduling — ensuring no critical moment is missed and your clinical team can stay focused on patient outcomes.
Seamless Operational Support04
ACT.360
A dedicated monitoring and data platform enabling long-term safety surveillance, real-world evidence capture, and structured outcome documentation - giving you and the broader clinical community actionable insights from every patient's journey.
Real-World EvidencePublications
Read our publications, published in prestigious journals such as The Lancet Haematology, Molecular Cancer Therapeutics by AACR and Blood by the American Society of Hematology.
Enabling access to talicabtagene autoleucel in relapsed/refractory B-cell malignancies; multicenter real-world evidence on delivery, efficacy and safety
Article
July 16, 2026Blood Cancer Journal
Talicabtagene Autoleucel for Relapsed or Refractory B-cell Malignancies: Results from an Open-label, Multicentre, Phase 1/2 Study
Article
Apr 1, 2025The Lancent Haemotology
Excellent Safety Profile of a Low-Cost Novel Humanized CD19 CAR T-Cell Therapy, Actalycabtagene Autoleucel : Potential Impact on Access and Feasibility
Abstract
Dec 9, 2023American Society of Hematology Meeting

NexCAR19™ Prescribing Information Guide
Essential prescribing information and medication guide for NexCAR19™ (Talicabtagene autoleucel), a CAR-T cell therapy for treating relapsed/refractory B-cell lymphomas and B-cell acute lymphoblastic leukemia. Includes detailed dosing instructions, safety information, and patient counseling guidelines.
Partnered Hospitals
Our strong association with over 130 + leading cancer treatment hospitals in India ensures hassle-free treatment with our CAR-T cell therapies.
 Disclaimer: For the use of registered medical practitioners / healthcare professionals only.
Disclaimer: For the use of registered medical practitioners / healthcare professionals only. i) The content in this section is intended solely for scientific, informational, educational and promotional communication to healthcare professionals and is not intended for patients and the public.
ii) NexCAR19™ shall be used only in accordance with the locally approved prescribing information and applicable marketing authorization. Before prescribing, healthcare professionals should refer to the approved prescribing information for complete details on: Indications, Dosage and administration, Warnings and precautions, Contraindications and Adverse reactions. Additional information about the product shall be available upon request to ImmunoACT @ helpdesk@immunoact.com
iii) Content within this section may include information regarding products, indications, and clinical data that are approved only in specific countries or regions. Availability, approved indications, and prescribing information may vary by jurisdiction. Healthcare professionals should refer to local prescribing information and applicable regulatory requirements.
iv) If you become aware of any adverse event, suspected adverse reaction, product quality complaint, or special situation (e.g., use in pregnancy, medication error, overdose) associated with NexCAR19™, please report it promptly to ImmunoACT at pharmacovigilance@immunoact.com
v) The information provided is for general scientific and educational purposes and does not constitute medical advice or a recommendation for any particular patient. It is not a substitute for the independent professional judgment of the treating physician, who remains solely responsible for treatment decisions based on the individual patient's condition and the approved prescribing information
vi) While ImmunoACT endeavours to ensure that the information on this website is accurate and up to date, it is provided 'as is' without warranty of any kind, express or implied. ImmunoACT does not warrant that the content is complete, current, or error-free, and reserves the right to amend or update it at any time without notice.
vii) All materials contained in this section are proprietary. Unauthorized reproduction, distribution, or disclosure is prohibited.